
Medical billing and revenue cycle management (RCM) are connected, but they are not the same thing. In short, medical billing focuses on claims and payments, while RCM manages the full financial lifecycle of patient care.
Medical billing vs. revenue cycle management: Medical billing is the process of preparing, submitting, tracking, and collecting payment for healthcare claims. Revenue cycle management is the broader system that manages the entire financial journey, from patient scheduling and eligibility verification through to coding, claims, denials, patient payments, reporting, and revenue optimization.
In 2026, with payer rules becoming more complex, prior authorization volumes climbing, and patient financial responsibility at an all-time high, it’s never been more important for healthcare organizations to understand the distinction between billing and RCM.
An understanding of these two functions informs how internal teams might mobilize and restructure to operate within the current challenges. It also provides valuable insights about whether your organization has gaps that would benefit from a billing partner, a full RCM partner, or a hybrid arrangement to support financial operations.
This guide walks through everything healthcare leaders, CFOs, billing managers, and practice administrators need to know about medical billing and revenue cycle management in 2026. We cover the operational differences, financial implications, compliance considerations, patient experience effects, and decision criteria related to optimizing each function.
What Is Medical Billing?
Medical billing is the process of translating healthcare services into claims and invoices so that providers receive payment from payers and patients. It is an execution-focused function that sits inside a healthcare organization’s financial management, but it does not define the organization's financial strategy.
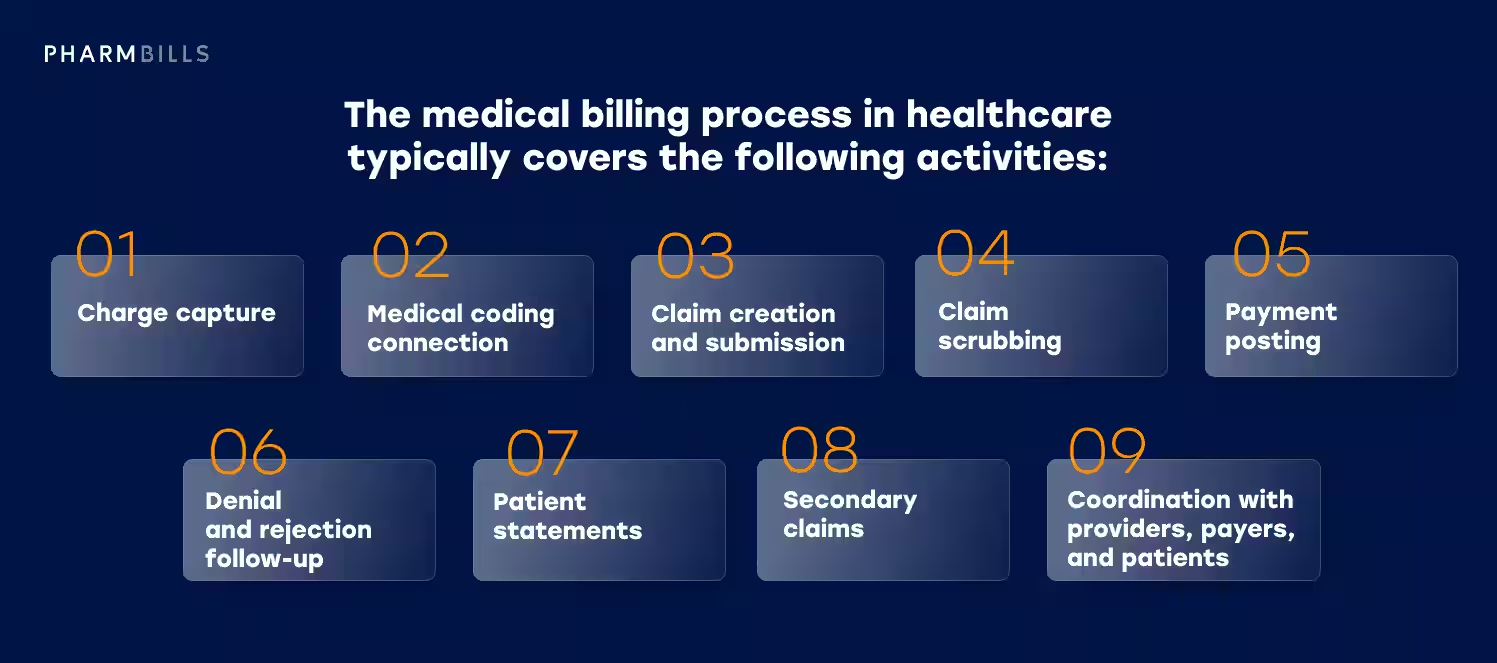
The medical billing process in healthcare typically covers the following activities:
- Charge capture. Recording every billable service rendered, with the supporting detail needed for accurate coding.
- Medical coding connection. Receiving coded claims from medical coders (or, in smaller practices, coding alongside billing) and validating that the codes match what was documented.
- Claim creation and submission. Building the claim per payer specifications and submitting it through the clearinghouse.
- Claim scrubbing. Running pre-submission edits to catch payer-specific errors before the claim leaves the building.
- Payment posting. Reconciling remittances, applying payments and adjustments to patient accounts.
- Denial and rejection follow-up. Investigating each denied or rejected claim, correcting where possible, appealing where warranted.
- Patient statements. Generating statements for outstanding patient balances after insurance has adjudicated.
- Secondary claims. Submitting to secondary and tertiary payers when applicable.
- Coordination with providers, payers, and patients. Handling questions, providing documentation, and routing escalations.
A useful frame of reference is that medical billing turns a documented encounter into collected revenue, but its scope ends with claim resolution. For example, medical billing does not own scheduling, eligibility verification, payer contracts, or patient financial counseling before the visit. Those activities are technically owned by RCM, which is why we sometimes talk about “RCM in medical billing.”
In 2026, medical billing is increasingly shaped by tighter payer rules, frequent coding updates, expanded prior authorization requirements, higher patient payment expectations, deeper software integrations across the practice, and an intensified compliance environment. Billing teams that keep up with these changes consistently outperform those that do not continually review and adapt their processes.
Related Services
Pharmbills supports healthcare organizations across the full billing lifecycle with dedicated billing professionals who work inside your existing systems. Learn more about our Medical Billing Services.
What Is Revenue Cycle Management?
Revenue cycle management is the end-to-end management of the financial lifecycle of patient care. Where medical billing handles the claim, RCM manages everything that determines whether the claim succeeds, and what happens to the revenue after it does. Put simply, RCM is the operational and strategic backbone of financial operations in healthcare.
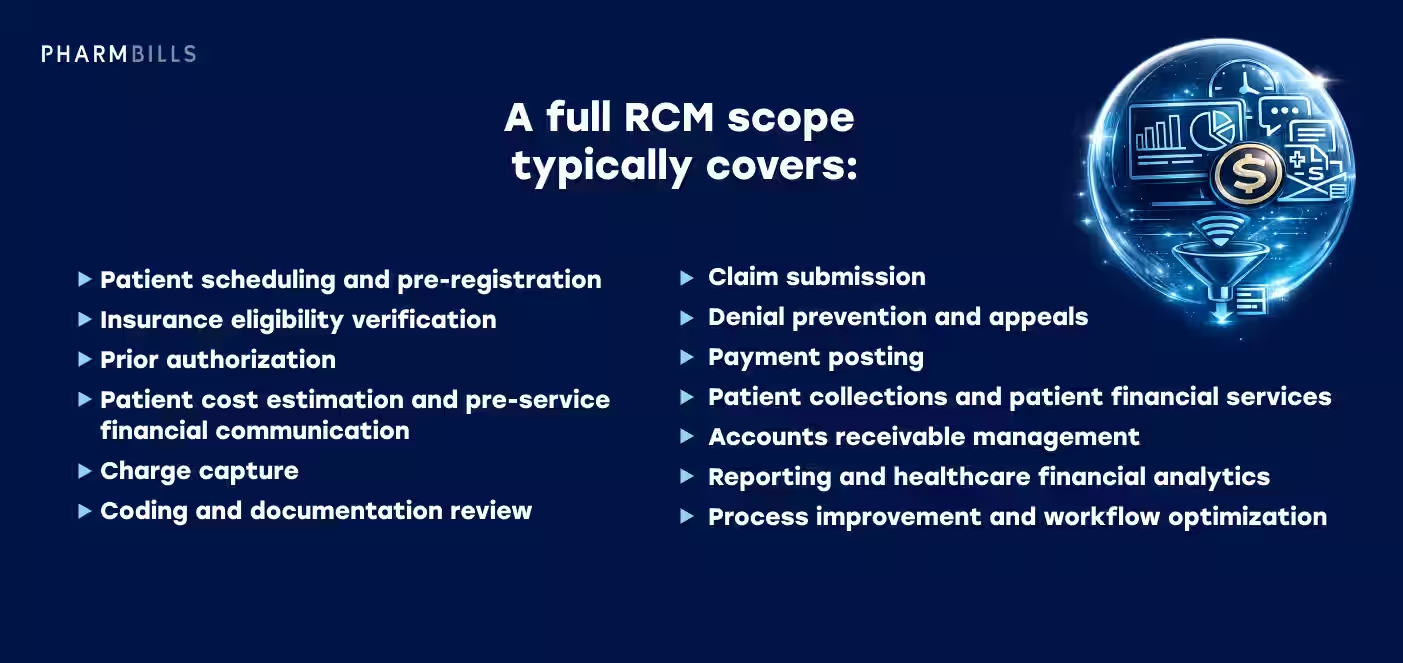
A full RCM scope typically covers:
- Patient scheduling and pre-registration
- Insurance eligibility verification
- Prior authorization
- Patient cost estimation and pre-service financial communication
- Charge capture
- Coding and documentation review
- Claim submission
- Denial prevention and appeals
- Payment posting
- Patient collections and patient financial services
- Accounts receivable management
- Reporting and healthcare financial analytics
- Process improvement and workflow optimization
The defining feature of RCM is its breadth. It connects the front office (scheduling, registration, eligibility), the clinical encounter (documentation, charge capture), the back office (coding, claims, denials, A/R), and the strategic layer (analytics, payer relations, compliance, KPI reporting). Done well, it functions less like a department and more like a discipline that runs across the organization.
How Does RCM Relate to Medical Billing?
The easiest way to answer the question, “What is RCM in medical billing?" is that billing activities are just one part of a larger revenue strategy. When viewed through an RCM lens, the billing function still does the same work it always did, but it operates inside a complete RCM system designed to prevent problems before they reach the claim, and to surface revenue leakage wherever it occurs.
That framing matters for healthcare leaders considering revenue support. When an organization evaluates whether they need a billing partner or a full RCM partner, the question is rarely about claim mechanics. It's about how much of the surrounding system the partner is expected to own.
Learn More
For organizations needing support across the full financial lifecycle, Pharmbills provides dedicated revenue cycle management services that integrate into existing workflows and technology.
Medical Billing vs. RCM: Quick Comparison Table
The table below provides a quick summary of the practical differences between medical billing and revenue cycle management.
Now, let’s take a closer look at the most important differences between medical billing and RCM in 2026.
Key Differences Between Medical Billing and Revenue Cycle Management
The real value of understanding the difference between medical billing and revenue cycle management shows up when you look at five specific dimensions: scope, timing, responsibility, strategy, and metrics. Each one shapes a different operational and commercial decision.
Scope
Medical billing handles claim-related processes, such as:
- Preparation
- Submission
- Payment posting
- Denial follow-up
- Patient statements
While the billing scope ends roughly at the boundary of the claim, RCM extends into the patient’s full financial journey, covering:
- Scheduling
- Eligibility
- Authorization
- Documentation
- Claim
- Payment (or denial)
- Collections
- Reporting
- Process improvement
When organizations describe revenue cycle management medical billing as a single integrated function, they are describing how RCM contains the entire billing workflow.
Timing
Medical billing often begins after care is delivered and documented. By the time a billing team sees a claim, the relevant clinical encounter is finished, the codes are assigned, and most of the upstream decisions have already been made.
RCM, by contrast, starts before the appointment. Scheduling, eligibility checks, prior authorization, and patient cost estimation all happen before any service is rendered. Most preventable revenue problems in 2026 originate in this pre-service window, which is one reason the medical billing revenue cycle conversation increasingly favors an integrated view.
Responsibility
Billing teams are responsible for clean claims going out the door and collections coming in. Their performance is judged on claim-level outcomes.
RCM teams carry a broader mandate. They prevent problems before they become denials, surface revenue leakage wherever it occurs, and improve the underlying processes that produce billing inputs.
A high-performing billing team can still report poor results if upstream eligibility or documentation is broken. In general, RCM owns those upstream conditions, while billing operates within them.
Strategy
Medical billing is largely transactional. It runs on volume, accuracy, and turnaround. RCM is strategic, analytical, and cross-functional.
RCM produces reporting that informs payer contracting, workforce planning, and capital decisions. Revenue teams also tend to own the relationship between operational data and financial planning, including healthcare revenue optimization initiatives that improve performance over time, not just claim-by-claim.
Metrics
This is where the difference between medical billing and revenue cycle management becomes most measurable.
Medical billing metrics tend to focus on the claim:
- Clean claim rate
- Denial rate
- Days in A/R
- Payment posting speed
RCM metrics include all of those, plus a broader set, including:
- Net collection rate
- Cost to collect
- Patient collection rate
- Prior authorization turnaround
- Revenue leakage by stage
A billing scorecard tells you how well claims are being processed. An RCM scorecard tells you how well the financial system is performing.
Where Medical Billing Fits in the Revenue Cycle
Medical billing is not separate from RCM. It is one of the core stages inside RCM, forming a critical execution layer that depends on every preceding step working correctly.
The typical revenue cycle flow looks like this:
- Patient scheduling
- Eligibility verification
- Prior authorization
- Patient registration
- Clinical documentation
- Charge capture
- Medical coding
- Claim submission
- Payment posting
- Denial management
- Patient billing
- A/R follow-up
- Reporting and revenue optimization
Medical billing concentrates around stages 8 through 12 — claim submission, payment posting, denial management, patient billing, and A/R follow-up. Coding (stage 7) often sits adjacent to billing depending on the organization.
Everything before stage 7 is RCM territory in the strict sense. Stage 13 (analytics and continuous improvement) sits at the strategic top of the cycle and feeds back into every earlier stage.
How Billing Is Impacted by the Wider Revenue Cycle
If earlier stages in the revenue cycle are weak, billing teams receive incomplete information, incorrect authorizations, poor documentation, or unverified eligibility. The claim that lands on the biller's desk is already compromised, and denials, delays, rework, and collection problems follow predictably.
This is why providers cannot solve all revenue problems by improving billing alone. Better claim scrubbing won't recover an MRI that was performed without prior authorization. Faster payment posting won't fix coverage that lapsed three days before the visit. Tighter denial follow-up won't reduce denial volume if eligibility is being checked once a week at scheduling and never again before the encounter.
Billing teams can do excellent work with the data they receive, but they don't generate this data — RCM does.
The Evolution of Medical Billing and RCM in 2026
Several shifts have changed how healthcare organizations approach the medical billing revenue cycle in 2026.
- More complex payer rules. Commercial and Medicare Advantage payers have expanded prior authorization lists, tightened documentation thresholds, and deployed AI-assisted claim review at scale. Billing teams who can't keep up with policy changes are starting denials from behind.
- Increased patient financial responsibility. According to the KFF 2025 Employer Health Benefits Survey, high-deductible health plan enrollment among covered workers reached 33%, up from 27% the year before, with average single-coverage deductibles at $1,886. Patients now represent a meaningful and harder-to-collect revenue segment.
- Stronger need for price transparency. Federal price transparency enforcement intensified through 2024 and 2025, raising the operational bar for estimate accuracy and good-faith estimate workflows.
- Prior authorization pressure. Physicians complete an average of 39 prior authorizations per week and lose 13 hours doing it. PA is now a structural drag, not an occasional friction point.
- Growth of automation and AI-assisted workflows. Automated billing in healthcare has expanded from claim scrubbing into eligibility verification, denial prediction, and patient communication. Tools alone don't fix broken processes, but they raise the performance ceiling for teams that have the fundamentals right. For a deeper look at how this is playing out, see Pharmbills' guide to AI in medical billing.
- Greater focus on denial prevention over denial reaction. The cost of working a denied claim consistently exceeds the cost of preventing it. Organizations are reallocating effort toward upstream denial prevention, which is RCM work, not billing work.
- More demand for real-time reporting. Monthly close cycles aren't fast enough to catch payer policy changes or staffing gaps before they cause a material revenue impact. Healthcare financial analytics is becoming a daily discipline.
- Higher expectations for patient-friendly billing. Confusing statements, surprise bills, and slow billing-question response times now drive patients away. Patient payment experience is a competitive variable.
- Continued staffing pressure in healthcare administration. Revenue cycle vacancies remain widespread. Most organizations are operating with smaller teams than they consider adequate.
- More interest in outsourcing and hybrid delivery models. Healthcare outsourcing (both partial and full) has expanded as a response to staffing pressure, technology gaps, and payer complexity. The choice is rarely "outsource everything." It's "outsource the specific functions where capacity or expertise is short."
Each of these shifts touches both medical billing and RCM, but they don't touch them equally. Payer rules and AI-assisted review affect billing directly. Prior authorization, transparency, denial prevention, real-time reporting, and the patient payment experience are predominantly RCM responsibilities.
That asymmetry is why the medical billing vs revenue cycle management decision has become more consequential. Billing-only support increasingly leaves more of the 2026 problem unaddressed than it did five years ago.
Why the Difference Matters for Healthcare Providers
Misunderstanding the difference between medical billing and revenue cycle management has real commercial consequences. The most common failure mode is that a provider notices revenue problems, hires a billing vendor expecting full revenue cycle improvement, and watches the same problems persist six months later.
In many cases, the vendor is doing its job competently, but the problems were never billing problems in the first place. The scenarios below show how this often plays out.
The difficult part in these scenarios is figuring out where in the revenue cycle the problem originated, so that it can be addressed.
Identifying Medical Billing vs. RCM Problems
RCM problems like slow cash flow, persistent denials, weak patient collections, and limited visibility frequently appear as billing problems, but the root cause usually sits upstream. Choosing the wrong service model means addressing symptoms instead of causes.
This is why the medical billing revenue cycle distinction matters as a sourcing decision. If your denials are concentrated in back-end mechanics (claim form errors, payment posting issues), billing services can absolutely move the needle. If your denials are concentrated in eligibility, prior authorization, or documentation, you need RCM-level intervention, regardless of how good a billing partner you hire.
Medical Billing Responsibilities in Detail
This section covers what a medical billing function, whether in-house or outsourced, typically owns as scope. The list is operational and execution-focused, in contrast with the broader scope laid out for RCM in the next section.
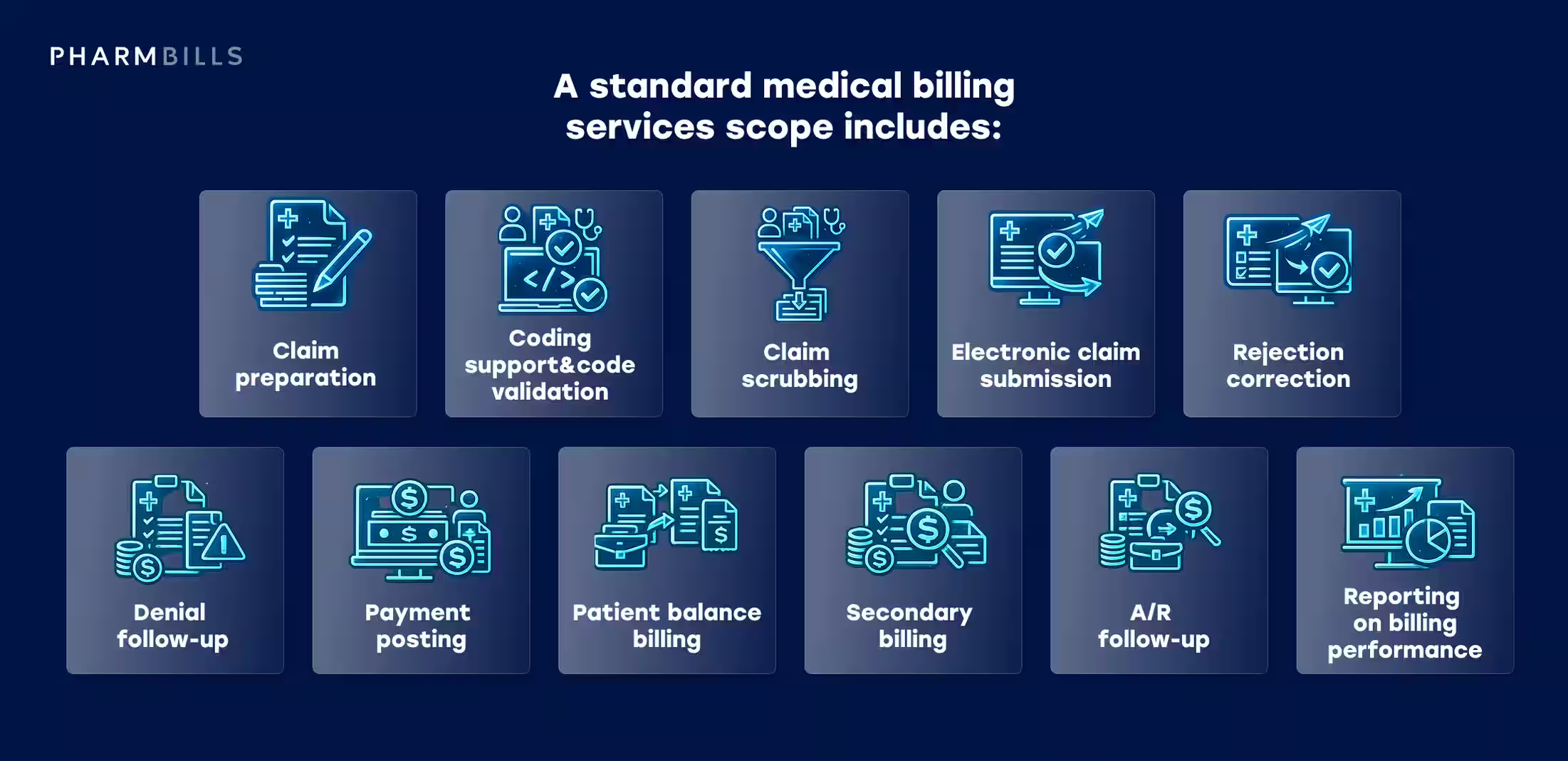
A standard medical billing services scope includes:
- Claim preparation. Building the claim from the encounter record, applying payer-specific formatting and coding rules.
- Coding support and code validation. Validating that coded charges align with documentation; querying the coder where discrepancies appear.
- Claim scrubbing. Running pre-submission edits to catch errors before clearinghouse rejection.
- Electronic claim submission. Transmitting clean claims through the clearinghouse to each payer.
- Rejection correction. Working clearinghouse and front-end rejections quickly to keep the claim moving.
- Denial follow-up. Investigating payer denials, gathering supporting documentation, filing appeals where warranted.
- Payment posting. Posting payments and adjustments from ERAs and paper EOBs against the correct accounts.
- Patient balance billing. Generating patient statements after insurance has finished adjudication.
- Secondary billing. Submitting to secondary and tertiary payers when coverage applies.
- A/R follow-up. Working aged accounts to bring days in A/R back to target and reduce write-offs.
- Reporting on billing performance. Producing clean claim rate, denial rate, days in A/R, and payment posting metrics for leadership.
The pattern across all of the points above is claim-centric execution. Outsourced medical billing services are typically a strong fit for providers who have stable front-office workflows, reliable eligibility verification, solid clinical documentation, and the patient access processes that produce billable encounters.
When those upstream pieces are working, a focused billing partner can deliver substantial improvement in claim accuracy, denial recovery, and A/R aging.
Additional Insights
For a deeper look at how outsourced billing partnerships work in practice, see our guide to the benefits of outsourcing medical billing.
Revenue Cycle Management Responsibilities in Detail
RCM scope is broader than billing scope by design. A well-defined RCM function, whether in-house at full capability or delivered through an outsourced RCM services arrangement, owns work across four layers. The lists below cover what each one is responsible for.
Front-end responsibilities. Everything that happens before care is delivered:
- Patient scheduling and appointment management
- Patient registration and demographic capture
- Insurance eligibility verification (ideally at scheduling and again at check-in)
- Prior authorization workflow management
- Patient cost estimation and financial counseling
Mid-cycle responsibilities. The clinical encounter and the work needed to translate it into a billable claim:
- Clinical documentation review
- Charge capture
- Medical coding and coding accuracy oversight
- Claim preparation and pre-submission edits
Back-end responsibilities. Claim submission through final payment resolution:
- Claim submission
- Payment posting
- Denial management
- Patient billing and patient collections
- Accounts receivable management
Strategic responsibilities. The analytical and process-improvement layer that runs across all three operational phases:
- Healthcare financial analytics and KPI reporting
- Payer trend monitoring and contract performance review
- Workflow optimization and process redesign
- Financial compliance in healthcare and compliance monitoring
- Forecasting and revenue planning support
The key takeaway is that RCM is about building a repeatable system that reduces preventable revenue loss over time, not just getting paid for individual claims.
The strategic layer is what distinguishes an RCM function from a billing function. It produces the reporting and process discipline that surfaces problems before they show up in the bank account, and it informs the operational decisions that prevent the next round of denials and delays. Strategy is also the piece most often missing when a provider has billing support but no broader RCM plan.
Deep Dive
For a foundational overview of how the revenue cycle works and why each stage matters, see our article What is Revenue Cycle Management (RCM) and Why Is It Important for Healthcare?
Front-End, Mid-Cycle, and Back-End RCM Explained
The phase view of RCM is one of the most useful mental models for understanding where revenue gets won or lost. Each phase has a distinct purpose, a distinct set of risks, and a distinct relationship to the billing function.
Front-End RCM
Front-end RCM is everything that happens before the patient receives care. The work here sets up every downstream process for success or failure.
- Scheduling captures the patient's intent to be seen and routes them to the right provider, location, and time.
- Registration collects the demographic and insurance information that every subsequent step depends on.
- Insurance verification confirms that the coverage is active, the patient is eligible for the planned service, and the practice understands the patient's benefits.
- Prior authorization secures payer approval for services that require it, before they are performed.
- Patient estimates translate that coverage information into a number the patient can plan around.
- Financial communication explains expected costs before the visit.
When front-end RCM is working, the encounter that follows is fully cleared. Coverage is confirmed, authorizations are in hand, and the patient understands their financial responsibility. When front-end RCM is not running smoothly, almost every downstream step inherits a problem.
Mid-Cycle RCM
Mid-cycle RCM covers the clinical encounter and the work needed to translate it into a clean, codeable claim. This phase determines whether the claim that reaches billing is clean or already compromised before submission.
- Clinical documentation captures the specificity needed for accurate coding, which everything downstream depends on.
- Charge capture records every billable service tied to the encounter.
- Medical coding translates documentation and charges into the standardized codes payers use to adjudicate.
- Compliance checks confirm that documentation supports the codes being assigned.
- Claim preparation builds the submittable claim with all required attachments and payer-specific formatting.
Mid-cycle is where many revenue problems hide. Documentation gaps, coding errors, and missing charges typically don't get noticed until they cause denials downstream, at which point the cost to fix them has multiplied. Strong mid-cycle RCM catches these issues at the source, not at the claim.
Back-End RCM
Back-end RCM is the phase most people think of when they say "billing." It is where claims management and patient collections actually live, and where the impact of upstream work becomes visible.
- Claim submission transmits clean claims to each payer through the clearinghouse.
- Payment posting reconciles remittances and applies payments and adjustments to the correct accounts.
- Denial management investigates each denied claim, gathers supporting documentation, and files appeals where warranted.
- Patient billing generates statements once insurance has finished adjudicating.
- Collections work the remaining patient balance through statements, payment plans, and follow-up.
- A/R follow-up tracks aged accounts and works them to keep days in A/R within target.
Clean front-end and mid-cycle work produces back-end results that look easy, while broken upstream work produces back-end work that looks impossible.
Done well, back-end RCM gets claims paid quickly, recovers as much denied revenue as possible, manages the patient balance experience clearly, and keeps aged A/R within target. Done in isolation from the rest of the cycle, it spends most of its time fixing problems that should never have reached the claim.
Phase Strengths and Partner Choice
The phase model is also why the answer to, "Do we need a billing partner or a full RCM partner?" so often depends on where the organization's actual problems live. Strong front-end and mid-cycle work with weak back-end execution means a billing partner may be enough. Strong back-end execution with weak front-end and mid-cycle means a billing partner probably won't help, and may make the gaps more visible.
Most providers in 2026 are dealing with a mix, which is why the conversation increasingly lands on full RCM or hybrid arrangements rather than billing-only.
Financial Implications for Healthcare Providers
The operational distinction between medical billing vs. revenue cycle management translates directly into different financial outcomes. Each piece of the cycle affects cash flow, working capital, administrative cost, and long-term revenue visibility in a different way.
The patterns of financial implications described in the table below hold consistently across organizations.
The headline point is that medical billing improvements primarily affect claim accuracy and payment speed. In contrast, RCM improvements affect the full financial workflow, from denial prevention to patient collections and long-term revenue visibility.
The right support model to use depends on provider size, specialty, payer mix, internal staffing, software stack, and where the current pain points actually live.
Common Signs You Need Medical Billing Support vs. Full RCM Support
A useful way to choose between billing services and full RCM support is to look at the symptoms. The two lists below capture the most common signs of each kind of problem.
You may need medical billing services if:
- Claims are being submitted late, or sit in a pre-submission queue longer than they should.
- Payment posting is delayed, leaving A/R inflated and account balances unclear.
- A/R is growing, particularly in the 60–90 and 90+ day buckets.
- Denials aren't being followed up consistently, or aren't being worked at all once they pass a certain age.
- Billing staff are overloaded — turnover is high, vacancies are open, or the team is unable to keep up with volume.
- Patient statements are delayed, confusing, or producing repeat patient inquiries.
- Coding and claim errors are frequent at submission, with clean claim rate dipping below the typical 85% benchmark.
You may need full RCM support if:
- Denials are originating from eligibility, authorization, or documentation problems — not from claim form errors.
- The practice lacks visibility into revenue performance, with no reliable reporting on denial trends or A/R aging by payer.
- Patient collections are weak, particularly for the portion of revenue tied to deductibles and coinsurance.
- Front-office and billing teams operate in silos, passing information across rather than collaborating on root causes.
- Prior authorization delays are affecting payer reimbursement, with claims denying after the fact for missing or invalid authorizations.
- Leadership cannot clearly identify where revenue leakage is occurring, or which workflow stages are producing the largest losses.
- The provider needs scalable financial operations — not just additional claims-processing capacity.
If the first list reflects your situation, an outsourced medical billing partner is likely a strong fit. If the second list is more accurate, billing support alone won't close the gaps, and full RCM is probably the right scope.
Patient Experience and the Revenue Cycle
Patient experience is now firmly part of medical billing revenue cycle management. Commonwealth Fund research on insured working-age adults found that 44% have medical debt, with nearly half of those owing $2,000 or more. The patients walking into a typical practice in 2026 are more financially stretched than they were five years ago, which is why patient financial services has moved from a back-office concern into a strategic one.
Confusing bills, surprise balances, and slow billing-question response times damage patient experience as much as anything that happens in the clinical encounter (and they directly affect collection rates).
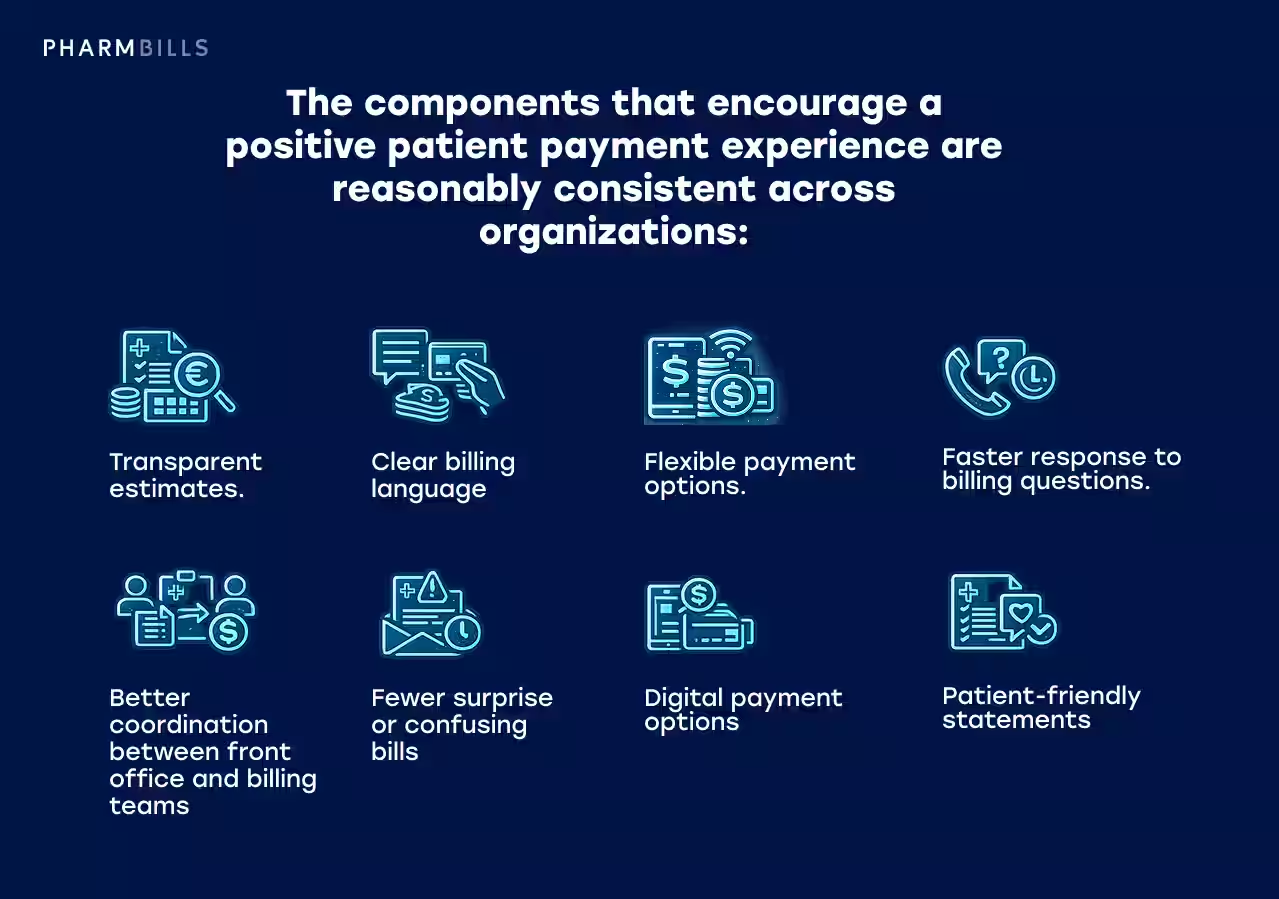
The components that encourage a positive patient payment experience are reasonably consistent across organizations:
- Transparent estimates. Accurate pre-service cost estimates that reflect actual coverage, deductible status, and likely out-of-pocket cost (not generic ranges).
- Clear billing language. Statements that a patient can read without calling for an explanation, with itemized charges and explicit explanations of insurance adjustments.
- Flexible payment options. Payment plans, financing arrangements, and digital payment methods that match how patients actually want to pay.
- Faster response to billing questions. Short queues, clear escalation paths, and resolution timelines that don't leave balances unresolved for weeks.
- Better coordination between front office and billing teams. Patients shouldn't have to repeat information across departments, and registration errors shouldn't quietly become billing problems later.
- Fewer surprise or confusing bills. Patients increasingly expect to know what they owe before they walk in, not weeks afterward.
- Digital payment options. Mobile-friendly payment portals, text-to-pay, and electronic statements as the default rather than the exception.
- Patient-friendly statements. Format, language, and structure designed for the patient (not for internal accounting convenience).
Most of these levers sit in RCM scope rather than billing scope. Billing affects the experience at the statement and collection stage, but by then the opportunity to prevent confusion has usually already passed. The pre-service stages where the patient experience is actually shaped (estimates, eligibility verification, financial counseling) are RCM responsibilities.
Technology, Automation, and Analytics in Medical Billing and RCM
Technology has reshaped both medical billing and RCM, but tools alone don't fix broken workflows. Software amplifies whatever process discipline sits underneath it, which is why the organizations getting real value out of automated billing in healthcare are typically the ones with the strongest fundamentals already in place.
The core technology stack across both functions typically includes:
- Billing software for claim creation, submission, and tracking.
- EHR/EMR and practice management system integrations that move charges, demographics, and coding data between systems without manual rekeying.
- Claim scrubbing tools that apply payer-specific edits pre-submission to catch errors before they cause denials.
- Eligibility verification tools that run real-time 270/271 transactions at scheduling and check-in.
- Prior authorization workflow tools that track status, surface upcoming expirations, and route renewals.
- Payment portals that support digital patient payments and flexible payment plan options.
- Reporting dashboards for clean claim rate, denial rate, days in A/R, net collection rate, and cost-to-collect.
- Denial analytics that segment denials by cause, payer, CPT, and provider (turning denial data into root-cause intelligence).
- Automation for repetitive administrative tasks like ERA posting, claim status checks, and routine appeals.
- Human oversight for exceptions, payer communication, compliance interpretation, and complex denials (the work that doesn't compress well into rules).
The underlying pattern is that technology accelerates execution while people interpret context. Automated billing in healthcare reduces manual touches on the predictable work, freeing skilled staff to focus on the exceptions and the cases that require judgment.
A common mistake worth flagging is that organizations sometimes assume buying better software will substitute for fixing process or staffing problems. It rarely does. The strongest results come from pairing capable technology with skilled people who know how to use it, which is where outsourced billing and RCM partners often add the most value.
More Information
For a thorough comparison of platform options across billing and RCM, see Pharmbills' guide Best Medical Billing Software in 2026: Reviews, Features & Pricing Comparison.
Compliance and Regulatory Challenges in 2026
Compliance affects both medical billing and RCM. However, RCM has the broader responsibility, as most compliance failures originate before a claim is created. In addition, the 2026 compliance environment is denser than it used to be, with active enforcement across several fronts and increasing payer-specific complexity layered on top.
Here are nine compliance areas every medical billing and RCM operation needs to track.
1. HIPAA and patient data protection
Administrative, technical, and physical safeguards across all handling of protected health information. The HHS Office for Civil Rights maintains enforcement activity and breach reporting. Failures here carry both regulatory and reputational cost.
2. Accurate coding and documentation
Coding accuracy isn't only a billing concern, it's also a compliance one. Documentation that doesn't support the codes submitted creates audit exposure regardless of payer.
3. Payer-specific requirements
Each payer has its own claim formatting rules, documentation thresholds, and policy update cadence. Tracking changes across the payer mix is an ongoing operational discipline.
4. Prior authorization rules and timelines
PA requirements vary by payer, by service, and increasingly by month. Missing a PA window or submitting the wrong supporting documentation is a structural source of denied revenue.
5. Price transparency requirements
Federal hospital price transparency rules remain in active enforcement, with civil monetary penalties issued for non-compliance and ongoing expansion of disclosure requirements.
6. No Surprises Act considerations
Open-negotiation tracking, qualifying payment amount verification, and good-faith estimate compliance affect both billing workflows and patient financial communication.
7. Audit readiness
Internal and external audits, whether payer-driven, OIG-driven, or self-initiated, require documentation trails that demonstrate accurate billing, supportable coding, and appropriate process controls. Pharmbills' guide to RCM audits walks through the process and what to look for.
8. State-level variation
State balance-billing rules, collection regulations, and licensing requirements layer additional complexity on top of federal frameworks, particularly for multi-state operations.
9. Source-backed compliance updates
Compliance is a moving target. Healthcare organizations need a reliable process for tracking rule changes and translating them into operational adjustments, not just reading bulletins after the fact.
Financial compliance in healthcare is a discipline that benefits from being treated as continuous rather than episodic. For a deeper look at how compliance checkpoints fit into the broader RCM operation, see our guide to HIPAA Compliance in Medical Billing.
Please note: This article is for informational purposes only. It is not legal, medical, or financial advice. Healthcare organizations should consult qualified compliance and legal professionals for specific requirements that apply to their operations.
RCM Medical Billing vs. RCM Metrics: What Providers Should Track
The metrics a provider tracks dictate how they can respond to financial challenges and optimize processes. Billing-focused metrics measure claim execution, while RCM-focused metrics measure overall financial performance. Both matter, but they answer different questions.
The table below summarises the most common KPIs and where they fit in the medical billing vs revenue cycle management distinction.
The top three rows are shared territory between billing and RCM. Billing-level work drives the immediate result, while RCM-level work shapes the upstream conditions that determine what that result can be. The metrics below that line are progressively more RCM-specific, as they track upstream activity or depend on cross-functional visibility that billing alone doesn't have.
In summary, billing metrics show how well claim execution is working, while RCM metrics show how well the financial system is working as a whole. A practice can have strong billing metrics and weak RCM metrics (usually a sign that the billing team is performing well on the claims it receives, even though upstream conditions are producing fewer clean ones than they should). But the reverse is harder to achieve, as weak billing metrics typically pull RCM metrics down with them.
Additional Insights
For a fuller exploration of this topic, see Revenue Cycle Management Metrics: Which KPIs Matter Most in 2026.
Outsourcing Medical Billing vs. Outsourcing RCM
Outsourcing has moved from optional to practical for many providers in 2026. The Bureau of Labor Statistics projects 15% growth for health information technologists and medical registrars through 2034, which means competition for skilled domestic talent will continue to intensify. For providers who decide outsourcing is part of the answer, the next question is what to outsource.
The choice between outsourced medical billing and outsourced RCM services comes down to scope. More specifically, deciding which parts of the revenue cycle the partner owns, and which parts stay internal.
Both models bring external capacity, but they solve different problems. Here's what each typically covers.
What Outsourcing Medical Billing Includes
A medical billing outsourcing engagement typically covers the execution layer of the revenue cycle, including the claims and payments work that follows from documented encounters.
- Claim preparation, submission, and follow-up
- Payment posting
- Denial management and appeals
- Patient billing and statement generation
- A/R follow-up
- Reporting on billing performance
What Outsourcing RCM Includes
A full RCM engagement covers all of the above, plus the upstream and strategic functions that determine whether the claim reaching billing is clean in the first place.
- Eligibility verification and prior authorization
- Patient registration support and pre-service financial communication
- Coding support or full coding services
- Healthcare financial analytics and KPI reporting
- Payer trend monitoring and policy intelligence
- Process improvement across front-end, mid-cycle, and back-end stages
When Each Model Fits
The decision usually comes down to where the provider's current problems live and what scope of help they actually need.
Outsourced medical billing may be enough when:
- The provider already has strong registration, eligibility, authorization, and documentation workflows
- The main issue is claim submission, denial follow-up, payment posting, or A/R
- The organization wants task-level billing support without restructuring the broader cycle
Outsourced RCM may be the better fit when:
- Revenue leakage is happening across multiple stages
- Denials are caused by upstream issues
- Leadership needs reporting and process improvement
- The provider wants a scalable financial operations partner
- Internal teams are overloaded across both front-end and back-end functions
Trade-Offs Between Outsourcing Billing vs. RCM
Each model has trade-offs. Billing-only outsourcing is faster to scope, lower in total cost, and easier to unwind if it doesn't work — but it leaves upstream gaps untouched.
Full RCM outsourcing addresses more of the revenue cycle, but requires deeper integration, more careful vendor selection, and active client oversight to avoid loss of visibility.
Common Risks and Mitigations

The risks of outsourcing without clear scope and reporting are consistent across both models. So are the mitigations. Here is a list of common risks to be aware of and how to stay ahead of them:
- Vague service-level expectations. Define SLA and KPI commitments in the contract.
- Opaque reporting. Require dashboard access and regular reporting (weekly or biweekly is a reasonable cadence).
- Communication lag. Establish escalation paths and response time commitments before the partnership goes live.
- Weak data security practices. Confirm HIPAA-compliant data handling and cybersecurity controls.
- Gaps in training or unclear handoffs. Map handoffs explicitly and align on onboarding and training expectations.
Real-World Outsourcing Outcomes
When the model and the partner are well-matched, outsourcing tends to function as a sustained extension of the internal team rather than a back-office vendor. One Pharmbills client described the outcome this way:
"We had a problem sourcing and retaining professional, skilled remote talent. Then we started working with Pharmbills and were extremely pleased that they delivered what they promised: smart, motivated people. As a result of having dedicated Pharmbills teams that mesh well with our culture, we've been able to markedly improve our collection rates. In just a couple of years, we've added a significant number of new team members. When we need to grow, Pharmbills gets the job done quickly and successfully."
More on RCM Outsourcing
For organizations actively evaluating full-service RCM partners, Pharmbills' guide to the Top Revenue Cycle Management Companies for Healthcare Providers in 2026 covers the vendor landscape in more detail.
Questions to Ask Before Choosing a Medical Billing or RCM Partner
Vendor selection is where a medical billing or RCM outsourcing model translates into actual capability. It's also where the difference between a partner that can solve the problem and one that can't becomes visible.
The starter questions below cover the dimensions that matter most when evaluating a candidate. For an expanded set with sample answers and red flags to watch, see Pharmbills' guide to questions to ask before choosing an RCM vendor.
Additional Reading
For organizations focused specifically on selecting a medical billing partner, our guide to How to Choose the Best Medical Billing Company in 2026 covers a detailed evaluation framework.
In-House Management of Medical Billing and RCM
In-house management of medical billing and revenue cycle management has real strengths, but it also has real challenges. Here’s an overview of the pros and cons of each.
Advantages of In-House Management
- More direct control. Leadership can prioritize, adjust, and intervene without going through a vendor relationship.
- Internal process knowledge. In-house staff develop deep familiarity with the organization's payers, specialties, and quirks.
- Closer communication with clinical and front-office teams. Coding queries, documentation feedback, and process changes happen across the hallway rather than across a contract.
- Easier alignment with practice-specific preferences. Workflow nuances, scheduling patterns, and patient communication norms can be tuned without external coordination.
Challenges of In-House Billing and RCM
- Staffing shortages. Revenue cycle roles remain difficult to fill across most U.S. markets. MGMA's 2025 polling flagged RCM vacancies as a persistent pain point even as clerical and clinical wages keep rising. Turnover is high, and replacement timelines are long.
- Training burden. New staff need months to reach productivity, and ongoing training is necessary just to keep up with payer rule changes.
- Software and technology costs. Healthcare billing software, EHR upgrades, clearinghouse fees, and analytics platforms add up.
- Compliance complexity. HIPAA, coding standards, price transparency, NSA, and payer-specific rules all need internal expertise to interpret.
- Limited scalability. Adding capacity means hiring, which is slow and expensive when it works at all.
- Difficulty covering vacations, turnover, or volume spikes. Smaller teams have less ability to absorb absence without performance impact.
- Limited analytics maturity in smaller teams. Building serious healthcare financial analytics capability typically requires investment that smaller organizations can't justify.
In-house management can work well for organizations that have strong systems, mature training programs, reliable oversight, and the budget to maintain all three. For practices that don't — particularly those running understaffed teams, dealing with persistent vacancies, or operating across multiple specialties or states — the case for some form of external support gets stronger each year.
Hybrid RCM Models: Combining Internal Teams with Outsourced Support
The hybrid model for medical billing revenue cycle management has become the most common choice for mid-sized providers in 2026. Most organizations don't actually pick between fully in-house and fully outsourced. They keep strategic oversight internal, while outsourcing selected execution-heavy functions.
The arrangement looks different from one organization to the next, but four patterns recur:
- The patient-facing split. Internal team handles patient communication; outsourced team handles billing and A/R. Useful when patient experience is a priority and back-end capacity is the bottleneck.
- The front-end / back-end split. Internal team manages registration, eligibility, and PA; outsourced partner handles claim submission and denial follow-up. Common when front-end is tightly tied to clinical operations but billing runs as its own discipline.
- The strategy / execution split. Internal leadership owns strategy and reporting; outsourced team provides execution support. Keeps decision-making close to the organization while expanding capacity.
- The capacity-flex arrangement. Outsourced team covers overflow, after-hours work, or specialized payer follow-up. Flexes with volume rather than committing to fixed-scope outsourcing.
The advantage of hybrid medical billing revenue cycle management support is that it preserves the parts of in-house management that produce institutional knowledge (relationships, judgment calls, clinical context), while bringing in scale, technology, and specialist capability where they're harder to build internally.
Hybrid is also the model that adapts most easily as the organization grows or its pain points shift, which is why so many providers are landing here rather than committing to a single approach.
Medical Billing vs. RCM: Which One Does Your Organization Need?
Which model fits depends on where your revenue problems actually start, what your internal capability looks like, and how much of the cycle you want to own day-to-day.
Choose Medical Billing Services If
- Your core problem is claims execution (claim submission, payment posting, denial follow-up, or A/R management)
- Your front-end workflows (scheduling, eligibility, PA, registration) are already stable and producing clean inputs
- You want operational support without restructuring the full revenue cycle
- Your denials are concentrated in back-end mechanics, not upstream causes
Choose RCM Services If
- Your revenue problems start before the claim is submitted (eligibility gaps, missing prior authorizations, documentation issues, or unclear patient estimates)
- You need help across upstream and strategic functions (eligibility verification, prior authorization, denial prevention, patient collections, analytics, and process improvement)
- You need reporting that surfaces where revenue is leaking and why
- Your organization is scaling, expanding into new specialties or states, or dealing with growing payer complexity
Choose a Hybrid Model If
- You have some internal strengths worth preserving but need support in high-volume or specialized areas
- You want to keep control of strategic decisions while improving execution capacity
- You need flexibility to scale support up or down without hiring or releasing a large internal team
- You're seeing problems in multiple stages but don't want to outsource everything at once
Most organizations in 2026 sit in the second or third group from the above list. The first one — providers with stable upstream operations who only need billing execution help — has been shrinking as payer complexity, staffing pressure, and patient financial responsibility have all increased.
The practical way to clarify which model fits is to look at denial root cause. Claim-form errors, posting issues, or appeals timing point to billing services being sufficient, while eligibility, prior authorization, documentation, or patient collections point to RCM.
Once the model is clear, the partner is the next decision. Pharmbills supports healthcare organizations with billing-focused engagements, full RCM, and hybrid arrangements, with experienced teams that work inside the client's existing systems.
The Bottom Line
Medical billing and revenue cycle management are connected, but they are not the same. Medical billing is a core function within RCM, acting as the execution layer that turns documented encounters into collected revenue. RCM is the broader system that covers the full financial lifecycle of patient care, from patient access through claim resolution and into analytics and process improvement. Understanding what each model covers (and what each one doesn't) is the difference between solving a revenue problem and treating its symptoms.
Choosing between billing services, full RCM, or a hybrid arrangement comes down to where revenue problems actually begin. If they begin at the claim, billing services are likely enough. If they begin before the claim — in eligibility, prior authorization, documentation, or patient financial engagement — RCM is the right scope. If revenue problems show up in multiple stages, a hybrid arrangement usually outperforms either pure approach. The denial pattern, the A/R aging picture, and the workflow stages producing the most leakage are usually the clearest diagnostic.
In 2026, this distinction matters more than it used to. Payer complexity has increased, patient financial responsibility has reached a multi-year high, automation and AI-assisted workflows have raised the performance ceiling, compliance enforcement has intensified, and revenue cycle teams across the country are operating shorter-staffed than they would like. Each of these shifts touches both medical billing and RCM, but they don't touch them equally — which is why the medical billing vs revenue cycle management decision has become a sharper commercial question than it was even a few years ago.
Considering Outsourcing?
If your organization is evaluating whether the answer is medical billing support, full RCM, or a hybrid arrangement, Pharmbills can help. We provide dedicated, trained professionals who integrate directly into your existing systems — Epic, eClinicalWorks, or whatever you already use — with zero workflow disruption and typical operational labor cost reductions of 40–50% versus domestic hiring. Our teams scale quickly when you need to grow, and our focus is on people and process, not on selling you new software. Contact us to discuss the right scope for your operation.


.avif)

![Strategies for Healthcare Revenue Cycle Optimization [2026]](https://cdn.prod.website-files.com/63d9425d235def15b898f020/662b859ab4ed0e9043c16de9_21826165.avif)

